La Avenida and Latinos in Recovery
Programmatic Requirements for Success, in the Words of La Gente
EXECUTIVE SUMMARY
There is no greater agony than bearing an untold story inside of you
- Maya Angelou
The Father Tracy Advocacy Center (FTAC), established in 2018, operates on North Clinton Avenue at the heart of the opioid crisis in Rochester. The Center’s mission is to help people recover from substance use disorders (SUDs) in a way that respects their dignity as humans and to advocate for services on their behalf. In support of this mission, FTAC collaborated with the University of Rochester Undergraduate Program in Public Health to interview women and men of the area on what they need to achieve sustained recovery. Trained interviewers conducted 28 open-ended, in-depth interviews.
The findings of this report are intended to help the FTAC and its partners advocate for culturally relevant recovery supports that are necessary for healing within this particular population, and that have historically not been adequately addressed by city, county, or private industry programming. Throughout the paper, the “population” will refer primarily to the women and men in the North Clinton Avenue / La Avenida neighborhood, and secondarily to the larger group of Latinos living in the City of Rochester.
In a departure from the national narrative, which shows the opioid epidemic as primarily rooted in over-prescribed opioids, the pathway to substance use among these participants was trauma and poverty. The distinctive origin of this population’s crisis emphasizes the need for programs that are expertly curated by the population itself.
Additionally, implementing appropriate SUD services for this population includes creating separate services for women (Latinas) and their specific circumstances. Using the dimensions of recovery outlined by Substance Abuse and Mental Health Services Administration (SAMHSA) and framing the suggested services within a biopsychosocial model, we present a holistic list of issues to be addressed. The recommendations of this report target community-level interventions to help build recovery capital: specific long-term resources in physical, social, human, and cultural capital that support people with SUDs through the complicated journey of reclaiming their lives.
ACKNOWLEDGMENTS
To all the participants, we are extremely grateful for your assistance in this most important project to transform the substance use community and conversation. On behalf of those listed below, we thank you.
Ethnographic Team Members
We are grateful for the hard work of University of Rochester undergraduate students in public health and anthropology for committing their time to attend training workshops, interview men and women, and organize the information for analysis.
Arnette Lovell
Ciara McGillivray
Kausar Haider
Mahima Joshi
Karina Garcia-Zarat
Simran Arya
Angela Benson
Nicolas Contento
Eleanor Esbrook
Carley Haft
Cameron Isaacs
Community-Academic Analytic Team
For 6 weeks, the combine analytic team met on Wednesday evenings to define codes, review transcripts, and discuss interpretations of the information. Their hard work is appreciated.
Rudy Rivera – Father Tracy Advocacy Center
Carlos Santana – Action for a Better Community
Florence Dukes – Helio Health
Nancy Chin – University of Rochester
I. Diana Fernandez – University of Rochester
Cameron Isaacs – University of Rochester
Ciara McGillivray – Father Tracy Advocacy Center
Additional Coding Support
Sasha Mesropov – Trillium Health
Funding
This work was supported in part by a Mini-Grant from the Center for Community Health and Prevention.
Additional Support
Members of the Common Ground Health’s Latino Health Coalition formed an Opioid Work Group that has met and worked together faithfully since 2019.
Rudy Rivera – Father Tracy Advocacy Center
Carlos Santana – Action for a Better Community
Lucia Colindres – Rochester Regional Health
Kristen Cushman-Smith – Ibero-American Development Corporation
Elisa DeJesus – Ibero-American Action League, Inc.
Janelle Duda-Banwar – Rochester Institute of Technology
Florence Dukes – Helio Health
Erin Egloff – National Council on Alcoholism and Drug Dependence – Rochester Area
Isabel Diana Fernandez – University of Rochester
Jeffrey Freeman – Common Ground Health
Julio Jordan – Ibero-American Action League, Inc.
Anne Kern – Monroe County Department of Public Health
Miguel Meléndez - Ibero-American Development Corporation
Mechelle Sanders – University of Rochester Medical Center
Tisha Smith – Monroe County Addiction Services
Van Smith – Recovery Houses of Rochester, Inc.
A special thank you to Lilian Ayala of Baden Street Settlement for her assistance and support in recruiting participants
INTRODUCTION
The Father Tracy Advocacy Center (FTAC), established in 2018, operates at 821 North Clinton Avenue at the heart of the opioid crisis in the city of Rochester. The Center’s mission is to bring people into recovery from substance use in a way that respects their dignity as humans, and to advocate for services on their behalf. Many health promotion programs first consult with people suffering with the disorder on how best to design services. People with substance use disorders (SUDs), however, are seldom consulted in fashioning services (McKay, 2016). FTAC wanted to change that and so collaborated with the University of Rochester Undergraduate Program in Public Health to carry out this work. Together we trained student interviewers to speak with woman and men in recovery. What we learned during these conversations warrants the development of services that meet the specific needs of the people in the North Clinton Avenue / La Avenida neighborhood. Our goal is to advocate for enhanced services that will support sustained, long-term recovery opportunities for this population.
Given the important differences in men and women’s experiences of drug addiction and recovery, we have addressed each group separately in this report, and summarized all recommendations in Table 2.
Ethnographic Approach
This was a quality improvement project intended to enhance SUD services for Rochester’s Latino community. We seek to promote and develop programs responsive to what these men and women identify as their most pressing problems. An ethnographic approach -- taken from anthropology -- centers people in recovery as the experts of their own experiences. Given the challenges in finding effective solutions to the rising problem of opioid addiction, we believe that directly asking people in the neighborhoods about their recovery process would reveal unique solutions. They told us their struggles. We listened carefully and transcribed their words. Then we analyzed what was said and examined existing literature, identifying what would meet their needs. [To be clear, they largely did not directly express specific ideas for how to design SUD programs.]
Interviews were open-ended, allowing the interviewee to control the direction and depth of their own stories. Interviewers’ main job was to listen to the respondent with minimal interruptions. As needed, the interviewers would ask follow-up questions to learn more about a particular experience or idea. Participants responded in the language of their choice, either Spanish or English. People’s stories were recorded with the permission of the participants (only 2 people refused). We generated verbatim transcripts of the stories.
A combined community-academic team analyzed the transcripts using the software Dedoos to identify and define recurring themes. We also looked at the structure of the stories to identify any patterns in the way the stories were told, what characters emerged, and what situational elements recurred.
What is Recovery?
The Substance Abuse and Mental Health Services Administration (SAMHSA) defines recovery as:
A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.
The four major dimensions that support a life in recovery are:
1. Health: overcoming or managing one’s disease(s) as well as living in a physically and emotionally healthy way.
2. Home: a stable and safe place to live.
3. Purpose: meaningful daily activities, such as a job, school, volunteerism, family caretaking, or creative endeavors, and the independence, income and resources to participate in society.
4. Community: relationships and social networks that provide support, friendship, love, and hope.
Given that recovery is a process of change across several dimensions, we believe that any SUD programs need to go beyond the initial clinical interventions and include provisions for continued support. Successful substance use treatment must incorporate ongoing recovery programming and mental health care.
Using a Biopsychosocial Model
We used a biopsychosocial (BPS) model to frame our thinking around recovery. The BPS model sees health as residing at the intersections of biology, psychology, and society. Using a BPS framework prevents us from taking a reductionist approach that focuses just on the biology of recovery. It expands our inquiry into the complex social and psychological factors underlying recovery.
BPS also aligns with the holistic definition of recovery offered by SAMHSA. A healthy recovery through the lens of BPS and SAMHSA happens by building physical and mental well-being as well as economic and social supports in the home and community, so one can live a meaningful life.
Local Context: The Latino Community of Rochester, NY
The Latino population of Rochester dates back to the nineteenth century, although major growth did not occur until the mid-twentieth century, when Latino families formed tight-knit neighborhoods in areas such as Brown Square, Marketview Heights, and Upper Falls. Unfortunately, many of these strong neighborhoods were disrupted in the 1970s, in a phenomenon that parallels other stories of gentrification and minority displacement. For example, urban renewal efforts caused the demolition of a major Latino neighborhood near St. Bridget’s Parish. Demonstrating incredible fortitude, the community was able to rally and establish a new neighborhood, or barrio, surrounding a proud landmark of the community: St. Michael’s Church on North Clinton Avenue. This region, La Avenida, is the heart of Latino culture in Rochester today.
The total Latino population in the Greater Rochester area has seen considerable growth in more recent decades, and now exceeds 60,000 people. The 2017 devastation of Hurricane Maria brought nearly 7,000 Puerto Rican refugees to Rochester, and today, about 69% of the Latino community in Rochester is specifically of Puerto Rican heritage. Latino influences are reflected in area businesses and events, including the Puerto Rican festival, Rochester’s longest-running multicultural festival.
Despite demonstrable strengths, the community experiences systemic inequities that negatively influence health outcomes. Years of Potential Life Lost (YPLL) metrics, one measure of population health, differ significantly across zip codes in Rochester (Latino Health Coalition). The Latino Health Coalition has identified three zip codes of particular concern: 14605 (where FTAC is located), 14613, and 14621. The 14605 area has the second to highest YPLL at just over 10,000 per 100,000 population. In contrast, 14534, a wealthier suburb of Rochester, has just under 3,000 YPLL per 100,000 population. In the zip codes of concern, sixty-six percent of the families fall below 200% of the Federal Poverty Level.
Opioids and the Latino Community of Rochester
Another stark health inequity within this region is the rate of opioid use and overdose. In 2018, there were 1,133 opioid overdoses overall in Monroe County: an average of three overdoses per day (Monroe County Heroin Task Force). Among the lowest socio-economic status zip codes (SES1), the rate of opioid overdose is 166 per 100,000 population compared to 76 in the highest SES zip codes (4 and 5). In regards to race/ethnicity, Latinos have the highest rate of opioid driven emergency department visits in the Finger Lakes region both in 2010 and 2016, with white people close behind (Common Ground Health). The opioid epidemic disproportionately affects those in a lower SES, regardless of race; however, the Latino community that FTAC serves has the highest risk of opioid driven emergency department visits.
Due to the disproportionate burden of opioid addiction among Latinos, this is an obvious target for public health intervention. Our project goal was to identify the unique needs of this population through in-depth interviews.
MEETING THE TREATMENT AND RECOVERY NEEDS OF WOMEN
The 15 women who spoke with us were all in recovery from SUD at the time of our conversations. Of the 15 women, 7 identified as Latina (4 of whom spoke only Spanish); 1 woman identified as Black; the remaining 7 women were white. Women ranged in age from 32 to 62 years old. Each interviewee (from both the men and women) was given a unique study number in the order the interviews happened. We refer to direct quotes in this paper by labeling them simply with the number assigned to the interview.
Both the scientific literature as well as our conversations with women and men point to clear sex/gender differences in addiction and recovery (McHugh et al., 2018; Becker et al., 2017; Greenfield et al., 2010; Center for Substance Abuse Treatment, 2009). Treatment programs for women that recognize their unique needs are more likely to promote sustained recovery and overall health. Below we detail what we have learned from our interviews with women about their lives, their addiction disorder, and paths to treatment and recovery.
PATHWAYS TO SUBSTANCE USE AMONG WOMEN
Women told stories of significant neglect and abuse in their families of origin. Many had drug-addicted parents who struggled to maintain an organized household for their children. They told of beatings, sibling suicides, incarceration, abandonment, and even premature death of their caregivers. Over the course of their childhoods, many women were either put in the care of relatives or sent to foster care, leading to feelings of abandonment. Some became caretakers of their younger siblings. Many were witnesses to violence during their childhoods.
I don’t wanna die like my mom died. I saw her die with a needle in her arm [and later in the story]… I don’t understand why my mom left me. #20
Some of our respondents reported receiving a diagnosis of Post-Traumatic Stress Disorder (PTSD). We know from the literature that women with a substance use disorder are significantly more likely to also have PTSD (Simpson, 2019; Bailey 2019). Many of our interviewees felt that unaddressed trauma impeded their ability to recover.
I feel like I have more support [in the recovery program] but the sadness and trauma that I have in my heart and mind doesn’t let me function to go forward. I see it everyday in my mind. All the abuse, everything that happened to me. I can’t forget. #20
Often they referred to drug use as a way of coping with their emotional trauma.
[I] got hooked on cocaine at the age of 20, 22 around there. And, I’ve been doing it ever since just to cope with not coping... #24
As they turned to drugs, women’s experiences of violence continued. Two of the women were kidnapped as teens. Some women were forced into sex work. They frequently became financially dependent on a male partner, leaving them vulnerable to physical, sexual, and emotional violence.
I been raped and everything… raped and shot… I was with this dude and I had some laundry. He was supposed to be taking me to the laundromat. Yes, the only thing he did he took me to [another city], and you might as well said he kidnapped me... And um, he wanted me to get out on the streets. That was my first taste of prostitution. You know, so, I told him I didn’t want to do it, at first. I told him I didn’t want to do it, and he beat me. He beat me so bad. #24
The women we interviewed reported being intermittently homeless during their use, further exposing them to violence, food insecurity, and sex work. One woman told us,
I lived in these streets. They are horrible. They are horrible if you are an addict... They are rock bottom... When I was living in them, I didn’t think there was another way. I thought this was where I was going to die. I would walk down the street and nobody would look at me or talk to me unless they wanted something from me. They wanted to give me a sample or try this or they were going to pay me for sex. #4
While many men report that their substance use began when injected by a friend, these women were often initiated into drug use through a male partner, sometimes without their consent. Substance use coercion (forced drug use) is a form of domestic violence that does not receive much public attention. Drug-facilitated sexual assault is rarely a one-time occurrence between intimate partners, and the women we interviewed told us that it is hard to stop using if your partner is still using. One woman thought of shared drug use as a way to connect with her partner and maintain their relationship:
...he had started smoking crack and we were not getting along, it was a very toxic relationship... I was like ‘Oh, well’ - here’s addict thinking - ‘we’ll smoke crack together and that will fix our relationship.’ So that was my thinking. That did not work at all. #8
PATHWAYS TO RECOVERY FOR WOMEN
Our interviewees told us that, as women, they are more likely than men to delay clinical treatment, generally because there is no one else to care for their children.
I know women are used to just carrying on the full load as far as kids, as far as, you know, um, the house. A lot of shelters, they don’t... accept single women because there’s always children following right behind them... I wish we would have a daycare here because I know a lot of people would come... I don’t know how it works, but if we had somewhere where they can keep their kids safely then they would be more open to come to programs... #19
Language isolation also deterred monolingual women from seeking treatment. Four of the women who spoke with us only spoke Spanish. One or two bilingual staff members at a treatment center will not meet the needs of a person who might need several weeks of inpatient treatment, if that person does not speak any English.
Women cited strong internal motivation as the major driver of initiating and completing treatment. Internal motivation sometimes came from a desire to regain custody of their children. Incarceration was sometimes the impetus to stop using substances entirely.
If I’m being honest, if an addict wants to change, you can’t force them to, then they don’t need treatment. You need to have strength to stop because a program can’t change that. When I got out of jail, I went to the women's home because I didn't have anywhere to live, I got clean because of my own will. I stopped using in jail. As I tell my friends in jail, no program can make you stop wanting to use. You have to make that choice. I apologize, I hate to say this. #18
[when we asked why she entered treatment] Cause of my kids, I’m trying to get my kids back. #26
[when asked about her son’s impact on her recovery efforts] Yeah cause at the end of the day nobody is going to treat mine like mine. Like if he go to foster care or he go to his grandmother's house or he go to a cousin's house; nobody going to treat him like how I treat him. #25
[I quit] because I had to, because I wouldn’t stop smoking from my pregnancy, they told me that CPS was going to take my baby and that they was going to put me into inpatient. Either or, I didn’t want that to happen. #25
A woman that has lived through and possibly continues to live with sources of trauma is likely to already suffer from poor self-image and self-esteem. If their education has been interrupted, or their dreams for a particular future seem unattainable, they may have a sense of hopelessness. They might seek substance use to avoid the pain they feel, or the situations they are in. Even when life as a substance user becomes unbearable, individuals may not be able to disentangle themselves from these multiple sources of trauma without considerable help.
Racial, gender, and language discrimination, are likely to intersect with housing problems, hate crimes, sexual harassment and assault, and even trouble with one’s own family of origin, leaving a woman convinced that there is no one who cares for her, or that she has no value to offer. It’s especially cruel when these forms of structural violence confront her as she approaches SUD treatment: facilities aren’t in geographically convenient locations; there are few or no bilingual staff or staff that have a similar background; publicly available insurance that may not cover the treatment that is needed. If, in fact, she is able to defeat all of these hurdles, she then faces – often alone – the need to find housing, work, and a community that will support her recovery. Our current regional systems are not structured in a way to help women heal and flourish. Structural violence is evident in the lack of necessary supports for this population, particularly as others in nearby privileged and white communities use the services designed for them with a comparable level of ease. The women we interviewed are aware of their lower-status in the eyes of the government and the community at large, and it’s another enormous barrier for incremental improvement in their lives:
It’s up to you to get the help. If you don’t go get help, they ain’t just gonna help you. You need to look for it. #26
When women do present for SUD treatment, they typically have more health problems than men. The women with whom we spoke listed multiple and significant physical health concerns: heart disease, diabetes, cancer, fibromyalgia, and lupus. Treating comorbidities can lead to more successful recovery as suggested in the SAMHSA definition of recovery as including good physical health. This requires that medical care for pre-existing conditions be part of a recovery program.
Given their repeated violent experiences with men, treatment and recovery might best be supported in women-only groups. Greenfield (2016) found a strong preference for women-only treatment groups among the women she was treating for substance abuse disorders. One of our women noted:
...they [the recovery program] made a group for women only. And, but it’s just one day a week. It’s just I can’t be around men. #27
Many women supported the idea for more groups for women only, stemming from the traumatic experiences they have experienced that were perpetrated by men. The women we spoke with often cited trouble talking to or around men (#26, #27). One interviewee suggested that women in leadership positions within the recovery centers would support positive transformations of the systems so programs better serve women’s unique needs. Female leadership would also be an incentive for women to enter treatment (#3, #19). In terms of logistics, some women recommended better transportation to facilitate a more convenient entrance to treatment, more job opportunities to keep people from drug-related commerce, and improved and more accessible English classes (#8, #14).
REORGANIZING LIFE: REDEFINING SELF-IDENTITY
Ten of the 15 women who spoke to us were in a formal recovery program, having recently abstained from substance use. The stories we heard from those women were considerably different from the men’s stories and significantly different from the women who had been in recovery for an extended time. The women who had recently begun treatment struggled to put together a coherent narrative. Their stories were disorganized, messy and confused. In her ethnography Addicted.Pregnant.Poor. Kelly Knight argues that women with substance use disorders operate in multiple ‘time zones’ (2016). She noted that women tended to parse time into several competing categories: addict time, housing time, jail time, treatment time, biomedical time, memorial time, and lifetime. This suggests that early in recovery, life and time feel terribly unmanageable. The recently recovering women struggle to keep track of what is happening at any moment. As a result, women in this stage of recovery will need ample time and support as they reorganize their lives into time zones that are not so disparate.
A significant source of support for reorganizing their lives can come from building new social networks that are healthy and drug-free. The women we spoke with craved human connections that would uplift them. Building reliable, healthy social networks takes time, skill, practice, and resources. Reinventing social networks with supportive people helps with abstinence, continued treatment, and recovery.
I stopped hanging around with people that I used to chill with and places... now I just be home. #26
There are [social] connections where it is almost like He [God] sent her to me. I know that sounds crazy but [my friend] has just lifted me up and vice versa. #4
...when I change my surroundings, like when I changed the people I hang out with, my behavior changed a lot. #19
What we have found in the literature is that women’s recovery can be supported by a redefinition of their self-identity. Rhodes and her colleagues (2018) conducted 30 interviews with women being treated for substance use disorders. They concluded that women’s desires to “shift their identities” and abandon a sense of self as a drug “user” stemmed in part from a strong desire to be a better mother, partner, and/or friend. That is, they were highly motivated to craft a new self-identity so they could create or repair valued relationships. Similarly, Kearney’s reanalysis of interview studies with women (1998) identified connections to others as a critical aspect of women’s recovery. Best (2015) points out that illicit drug use is the most highly stigmatized health condition in the world and that overcoming social stigma includes building social networks that can support a new, affirmative self-identity.
Especially relevant to this report is the research of Morse and her colleagues among women drug court participants in Rochester, NY (2014). They identified a need for female-specific recovery programs that support women's desires for enhanced relationships, physical health, trauma-informed treatment, housing accessibility, childcare, and employment.
RECOMMENDED SUD SERVICES FOR WOMEN
What participants told us is consistent with the scientific literature on women and their SUD treatment and recovery experiences. Many of our recommendations are in line with endorsed, evidence-based practices shared by SAMHSA. Based on these sources, we earnestly advocate for regional programs to provide an honest assessment of how they are or are not supporting treatment and recovery efforts that empower women in managing past traumas and living a healthy life after SUD. FTAC’s goal for established programs is to support the efforts of women in recovery as they “rescue themselves.” With that in mind, we recommend the following components be integrated into regional treatment and recovery programs:
1a) Direct Collaboration to Treat Mental Health
The importance of direct collaboration with mental health professionals to diagnose and treat mental illnesses and co-occurring disorders cannot be understated. Effective programs must address childhood trauma and later adult trauma to support recovery. Viewing mental health and SUD as an intertwined package will lead to a more holistic and long-term successful recovery.
Women often experience multiple complex traumas over the course of their lives.
1b) Direct Collaboration to Improve Physical Health
Direct collaboration with primary care providers to diagnose and treat comorbid physical conditions is essential. Simple referrals are insufficient.
Women in this population have not historically been given the skills or assistance to navigate insurance and health systems. Women also need to be taught how to manage chronic health conditions, proper nutrition, and the importance of regular exercise.
1c) Develop a Healthy Relationship with Oneself
Building life skills and coping skills will help an individual to develop a more positive outlook for the future and serve as a protective factor against relapses.
Teach women to use positive thinking and words that reinforce recovery, and help them learn identify when they are using negative language in reference to themselves by asking “what are the things you say to yourself?” Support habits that use their own words as encouragement and build self-confidence to become their own “cheerleader.”
1d) Develop Skills for Healthy Relationships with Others
Cohabitating relationships such as those with children, intimate partners, and/or others are critical in remaining abstinent from substances, as “home” should be able to be a safe place of refuge. Other relationships with regular interactions may need to be repaired or developed, such as with other family members, friends, coworkers, employers, or neighbors.
Women who have experienced trauma caused by men may need additional assistance to learn how to identify abusive behaviors.
1e) Plan for Community Reintegration
Recovery management needs to extend beyond the traditional treatment programs and actively help people to reintegrate into communities and workplaces as well as build health social networks. Programs should teach skills for developing relationships with people that support recovery in actions and words; educate practical ways to dismantle old networks linked to drug use; and promote the repairing of social relationships with important people.
Peer services and mentorships can have a valuable place in this process, particularly for women, whose family pressures and trauma-related burdens pose additional challenges to abstinence.
1f) Implement Affordable and Accessible Childcare
Lack of childcare often acts as a barrier to entering and/or continuing treatment and recovery programming.
Having easily accessible day care services supports mothers and can alleviate an enormous mental and financial burden that can impede treatment and recovery. (We recognize this can also be a barrier for men and include it here as it is primarily an issue that, historically, has affected women most directly.)
1g) Provide Women-Only Programs
The unique biopsychosocial needs of women and frequent violent histories with men merits targeted, tailored programs specifically for women.
Table 1 shows these recommendations in relationship to the SAMHSA dimensions of recovery.

The recommendations in Table 1 are specific to women. In the full table of recommendations at the end of this report, we include additional elements to be applied to all SUD programs.
MEETING THE TREATMENT AND RECOVERY NEEDS OF MEN
We interviewed 13 men from the same neighborhood area, ages 23-68. All were either in recovery from substance use or planning to enter recovery. All were Spanish-speaking, and six chose to be interviewed in English.
The interviews demonstrated that there was a great deal of difference between the experiences of women and the experiences of men when it came to substance use. For instance, men are more likely to be introduced to drug use by a friend, rather than an intimate partner. Men’s stories also included reports of parents or older siblings who themselves suffered from SUD. Many men came from working class families that had trouble financially supporting their household. Selling drugs, a common way to be introduced to substance use, often served to supplement the household income.
PATHWAYS TO SUBSTANCE USE AMONG MEN
Most of the men we interviewed began their stories in childhood, recounting their difficulties growing up. In many cases, their fathers were absent.
The family I was born into… my parents were addicted. My father was an alcoholic. My mother was an alcoholic... They used a lot of alcohol and drugs. #9
I was nine years old then... they [his caretakers] were always beating me, abusing me. Kicking me, punching me. There was a bunch of things that really, now I understand that they were bad. Then I grew up with this hatred inside of me. #28
It was painful. I was mistreated physically, mentally. I was tortured. They hit me a lot. When a woman gets together with a man, when the kids have a stepdad, and he doesn’t see him as a kid but as an enemy... The kids suffer. I can’t forget any of these things. The father is an important part of a child's life. This marked my life. I am tired of life. I don’t want to live, many times [I thought of suicide]. My childhood was hard, sad. #11
Well, my family is a hard-ass family. Like you know they’re not an emotional family. Like you can’t really… show emotion. They just don’t know how to react to it. I was basically raised as if you showed emotion you were weak. So I never really showed my emotion even though it was beating me inside. I just never showed it. So I just kept it down. The reason how I kept it down was doing drugs... I mean when my grandfather passed away I did over probably a half ounce of coke down in the basement of my dad’s house by myself. I didn’t leave the basement for like three and a half days or something like that. #15
Often these families were desperately poor, and felt direct or indirect pressure to contribute to their family’s income or simply enjoy a brief thrill, such as in this example:
From time to time you got tired of eating bread soup, and - I started hustling when I was 10 years old. I remember selling joints for a dollar- that would give me that chicken leg, that cube steak, or pork chop. #5
I was raised without a father, so I had to work since I was little... I used to cut sugar canes, I used to shine shoes to make 15 cents. I harvested coffee beans. From my time as a youngster, I had to work, study and help my mother raise my brothers and sister. I would have to change my brothers’ diapers, and back then we had to do it the old-fashioned way. I started sniffing glue. It was not easy. I had to study, work. To help my mom and support my siblings. Take care of my siblings. Because I’m the oldest. #10
Interviewee #2 was raised by a single mother who was very proud when he became a manager of a big box store at age 19. Unfortunately, he sustained a serious back injury at work. He told us:
I got a really strong pain in my back and this doctor… prescribed to me Percocets. And I started taking them. And then I started, you know, feeling bad when I was not using it because they are opiates and I didn’t understand that in the moment. I just thought it was like a cold or something. But … and somehow I started realizing that I need these pills to work normally again. And then he take it off of me after like five months.
It is important to note that this is the only man we interviewed who became addicted to opioids because of prescription medication. All of the other participants started with street drugs and/or alcohol, not prescription opioids.
THE DRUG LIFE
Many of our male respondents reported that they began using drugs in their early teens.
I started drinking at 9. I found a cigarette at 9. At 13 I experimented with marijuana. #11
I was 14, that was the first time when I tried heroin. From the age of 14 all the way to the age of 39, I did heroin. I went through hell. #5
My first substance was at the age of 14, cigarettes and alcohol. At 16, I tried heroin and cocaine. #6 I tried marijuana at 13. My friends were older, they were in their twenties, thirties, and forties. They were always older than me, the friends that I hang around with. Then I smoked marijuana, I drank alcohol. It got from bad to worse. Got worse, then I tried other drugs, stronger than marijuana. #28
I was twelve years old when I started experimenting with drugs. #13
There are aspects of the drug life that the men found attractive, fun, and compelling. While the quantity of drugs sold vary substantially from person to person, the increased income does have an impact, even if it’s on the smaller end of the scale, such as selling dime bags. Other times, the income from drug dealing could be considerable and some men indulged in luxury items that had been out of reach of their families of origin. One man described it as
...Easy money. [It gets you] the girls, the fancy cars, good clothes, the jewelry, and... travel. #1
…I thought the lifestyle that I was living was awesome at that time because I was a teenager. That’s what it felt like. It felt like a really good feeling to where I was. It made me happy... So I kept doing it and doing it and doing it. And doing it. #15
If using drugs was a way to cope with previous trauma, the drug life compounded the trauma for many of these men and the SUD cycle began. One man referred to it as “the double problem;” you use drugs to make your problems go away, and then you realize that addiction was just another major life problem to manage. Life Skills Training on problem solving and coping through trauma would be beneficial to recovery.
It is a double problem because, I am trying to fix one problem, but what I do is make it worse...I am avoiding the problem by doing heroin, but that does not make the problem go away. The problem continues in the same way...and now I have another problem on top of it all--the need to keep using heroin. You understand? #13
Relapses are a regular part of the stories that these interviewees told. They generally described their relapses as a result of being triggered by an upsetting situation. One man told us about a relapse after he lost visitation with his daughter:
It’s a year and a half that I don’t see my daughter. It’s eating me like cancer. It’s destroying me. Like drugs and alcohol. It was that pain I was trying to cover from the drugs. I was trying to escape that reality. That was one of the triggers. #28
Another man relapsed when he became homeless:
…when I got released [from prison] I went [to] Rochester, New York... I have family over here... And when I got here, I started... living with one of my family. There was a problem living with my family because me, coming out of jail... People was kind of leery. “Oh, what was this guy in jail for? You know, a pedophile? Or this and that?” So I was living with my brother and my sister-in-law for a little bit. And then they kicked me out. I said, “Well, my God, what am I gonna do?” That was one of the reasons why I wound up doing drugs and hanging out. I don’t use that as an excuse but I believe that’s one of the things that triggered me to use drugs. #7
Eventually, many of the men saw that their lives using and/or dealing substances had devolved into pain and despair.
...sooner or later, it’s going to get you in prison, or get you killed, you know... But the lifestyle is very dangerous, you know. It was hard for me to fall asleep. It was like, one eye open and the other one’s closed. I had to protect myself and that took me to many different places in my life. #1
My experience with drugs has been horrible. All of my desires. It has affected my brain, my nerves, I have a mountain of pain in my bones. Not just for the drugs, but for my physical health. It has destroyed everything. #11
The addiction took everything I had... I tried to kill myself a few times. It was the depression. It’s a demon, a destructive demon. When a person falls into depression you have to seek help desperately. Addiction and depression is horrible. It takes the life from human beings. And I needed to seek help. #28
THE DECISION TO RECOVER
The decision to enter treatment often happens multiple times, as does the decision to leave treatment prematurely. According to the men who spoke with us there were many events that can prompt them to seek treatment and a release from what one man called “the prison of addiction” (#28). These reasons include fear of arrest and prison, near-death experiences (either theirs or someone close to them), and/or a desire to reconnect with their children.
...when they [the courts] offer me 9 to 12... I said oh my God this is serious now. And I changed a little bit... I don’t want to go back to that place. The time that you lose never comes back. Then I decided to change my life. #28
You feel so bad about yourself. You feel so unhappy. That’s what it does, the drugs do to you. They destroys you. And that’s why I changed my life. I felt so empty and miserable. Yeah I wanted to change my life and I went back to God because he’s the only one that knows everything in life. #28
One 68-year-old man attributed his decision to enter treatment to an emergency room doctor who gave him counseling:
You never find an [emergency room] doctor that will take his time and sit down with you. [The one doctor who did sit with me said] “You know, if you continue using drugs you’re gonna die. You know, why don’t you leave that alone? I’m looking at your medical records; you OD’d almost more than seven times already. So how much longer that you’re gonna continue doing that? One day you’re gonna fall and you’ll never gonna get up again.” So I believe in my heart that had something to do with me being clean today for two years. Because of the conversation that I had with that doctor. Because I got scared. #7
LIFE IN RECOVERY
Relapses and incomplete treatment efforts are common, and there are countless reasons that a person might view as a setback.
...a reason why a lot of people don’t recover when they go in the outpatient programs is because a lot of the counselors are… straight from the book, and just reading what they see in the book. They don’t experience being out in the streets or being homeless or selling your body and doing this other stuff. So. #15
Talking with a non-judgmental peer recovery professional who relates to them because they’ve been through similar circumstances supports a person’s recovery. People on La Avenida find these conversations at FTAC. Mr. Rivera himself is such a peer.
…a lot of places the reason why people don’t like going back is because they get judged. We don’t judge nobody because we’ve been there. We know that feeling. We know that feeling of being judged and it’s just not a feeling that you feel like you’re happy. #15
Life in recovery is a continual struggle, as Interviewee #2 notes below. He explained his on-going distress as not just psychological, but an embodied experience. Mental illness diagnoses and treatment are a critical part of the process for SUD treatment and recovery, as depression or anxiety – among many others – are often present as co-occurring disorders. For instance, while Interviewee #2 was no longer substances, it was difficult to get his body to respond to his attempts to motivate himself:
Withdrawal is difficult but [even after withdrawal is over] everything is out of control. You never enjoy anything. You know, you want to cook. Well, you don't feel like you want to. I love to cook and when I cook for my family, I enjoy making it good. But you don’t feel again like you want to do anything. All the time you’re just angry or sad. [For] months. You gotta wake up and motivate yourself every morning and for everything you’ve got to be motivating yourself really strong…I don't think it’s psychological because I’m really positive – [but] even when you are really positive about things…You don't feel energy. You don't feel moods. It’s not like it used to be. #2
The men themselves cited treatment from a mental health specialist for regular therapy as important to their treatment and recovery:
I gotta go to therapy because they find out that I was suffering from some kind of depression of being alone; the doctors recommended for me to see someone so I could talk to. #7
Most men saw the need for a holistic approach to sustained recovery:
Interviewer: In addition to therapy, what do you do to support your recovery?
I talk to Rudy … And I see a doctor once a month…Oh, and I work. I have a part time job that I work every afternoon. Most of the time I stay in my apartment. Alone. Watching television. And reading. Because I like to read a lot. #7
RECOVERY CAPITAL
A number of researchers have used the term ‘recovery capital’ to describe the resources essential to promote a sustained recovery (Hennessy, 2017; Zschau et al., 2016; Herbeck at al., 2014; Boeri et al, 2016; Cloud & Grandfield, 2008). Recovery capital includes physical capital (resources ranging from housing to cash to transportation and the like), social capital (social network structures), cultural capital (class-specific social practices), and human capital (skills, knowledge, and experience). Recovery capital is not the property of individuals, but a feature of communities (Zschau, T., 2016). Interviewee #11 provided a list of community-level supports that correspond to this idea of recovery capital:
Interviewer: [What is important in sustaining recovery?]
Interviewee: Information, vocational help, chat, movies. How to be a better father. Projects that help others. Supporting one another, these things. #11
A ROLE FOR THE FATHER TRACY ADVOCACY CENTER
Almost all of the men we interviewed had direct experience interacting with the Center and offered ideas on how the Center could better support recovery:
I think the Center is very good because there is someone who is always around to resolve our problems. He tries to solve your problem as much as he can. #13
Interviewer: So what do you think the Center can do to improve and help people?
Interviewee: For me, it would be good to try to communicate with people, run small groups to keep our mind busy with positive things. To use our intelligence for positive things instead of negative things. The Center is able to help more people, and people can come in and talk. You help others by virtue of your own experiences. #10
Interviewee #10 references the assets that people in recovery could bring to the work in the larger community -- specifically, experience and intelligence -- as well as the creation of a new identity as people who can do work that is both meaningful and produces change for the better for others.
Interviewee #6 also mentioned the Center:
Interviewer: Can you describe your daily routine?
Interviewee #6: The routine is usually three days a week that I go to groups, from 10:30- 12:30. Usually after that I come here to the Center. I like it because one feels comfortable and you feel welcome.
Interviewer: What aspects of the Center make you feel comfortable?
Interviewee #6: In all aspects, the people that come, what they offer. Usually on Friday they have food. People don’t have too many options. So they offer nutrition and make them feel comfortable.
Interviewer: Is there anything you haven’t liked?
Interviewee #6: No. They know what people have been through and where you come from.
Interviewer: Have you ever been to FTAC?
Interviewee #28: Yeah, they got good service. They care about the people who don’t have anybody to take care of them. Destitute. Church and institution, religion, they should put this in their brain to work together as brothers.
RECOMMENDED SUD SERVICES FOR MEN AND WOMEN
Analysis of the interviews, the existing literature, and the group’s knowledge and experience of this population led to recommendations, some of which are similar to those mentioned previously in the section on the treatment and recovery needs of women. Like those, they are in line with evidence-based practices, and we advocate that regional treatment programs provide an independent assessment of how they are or are not supporting treatment and recovery efforts that holistically care for men in this population whose needs go beyond an initial clinical intake. In that spirit, FTAC’s goal for our local, established programs is to support the efforts of this population of men as they seek to heal and utilize services that can assist them in moving toward a peaceful, healthy life. Therefore, we recommend that the following components listed in Table 2 be integrated into all regional SUD treatment and recovery programs.
2h) Provide Mental Health Literacy Training
In order to provide context and life-long skills to benefit themselves as well as those around them, programs should teach how to develop and maintain a regular mindfulness practice as well as a variety of coping mechanisms and basic mental health literacy information, including symptoms of common mental illnesses, available community resources, and frequently used terms such as triggers, trauma, depression, and anxiety.
2i) Increase Peer Counselor Workforce and Education
Peer counselors provide an important service to those in SUD treatment and recovery, and the impact is emphasized when the peers are of a similar background to the individual in treatment and can relate to their direct and indirect struggles.
2j) Ensure Language Access
2k) Provide Safe and Reliable Transportation
2L) Secure Adequate and Affordable Housing
Join forces with other organizations to advocate for the necessary expansion of Section 8 Housing in neighborhoods where drug use is not prominent, in new and positive environments that are gratifying for the families that live there.
2m) Address SUD and Mental Health Stigma
A community level intervention is needed to reframe substance use as a treatable illness instead of a moral failing.
Table 2 shows these recovery recommendations as they relate to the SAMHSA dimensions of recovery. Those recommendations that intervene at the level of the community, rather than at the individual level, will require cooperation, input, and dedicated financial resources across health systems, law enforcement, and local government, as well as private organizations like FTAC.
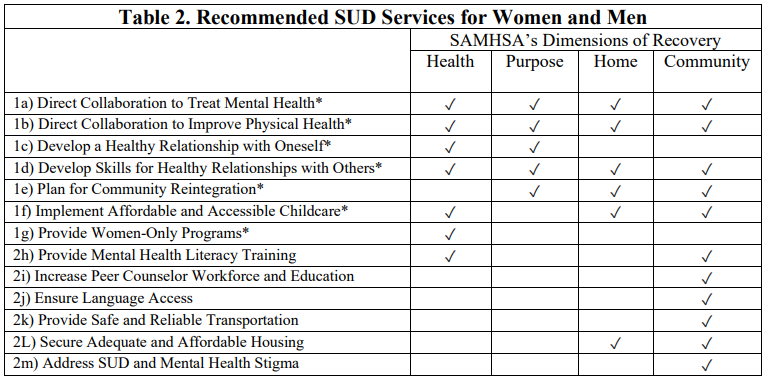
* see details for these recommendations in section titled “MEETING THE TREATMENT AND RECOVERY NEEDS OF WOMEN”
CONCLUSION
The women and men with whom we spoke suffer in varying degrees from multiple, complex traumas including persistent poverty, homelessness, violence, incarceration, lack of education, linguistic isolation, and estrangement from supportive social networks. They grapple with the significant social stigma attached to illicit drug use and incarceration. Nearly all started using street drugs as a response to dire social circumstances, not because of over-prescribed painkillers as in other neighborhoods. Because of this essential difference, SUD programs that primarily cater to other demographics are missing key components that are essential to the community of men and women that we work with.
Substance use has devastated these people, and there has been a lack of coordinated effort by those with financial resources to lift this population and its children out of the darkness of their traumas and into the light that shines on other, nearby, populations. It is time to right that wrong, and support all our citizens, especially those in our most vulnerable areas, such as the North Clinton Avenue / La Avenida neighborhood.
Struggling through Adverse Childhood Experiences (ACES) in childhood and adolescence, such as having a mentally ill caretaker, witnessing violence, and/or suffering sexual abuse, are known to result in a significantly higher risk for substance use in adulthood (Felletti, et al 1998). The childhoods our participants described were saturated with such traumas, and it is not at all surprising that they developed chronic substance use disorders. Current recovery programs are not working for this group of people. Their circumstances require a more holistic, long-term approach to recovery.
By listening carefully to these stories, we believe that our recommendations need to be considered as local SUD programs look at their program offerings and honestly evaluate which modalities can be developed or adjusted to meet the needs of this community. Are these programs truly language-accessible, or is there simply a translator on call from a national service? Do individuals in treatment and recovery understand the role that their childhood traumas have played in their alcohol and drug use? Will a man without family or supportive friends be able to find his own housing that won’t require him to walk through an open-air heroin market? Is a woman in group therapy being re-traumatized by sitting across from a person who is friends with her former abuser? Are we following guidelines that don’t include restorative functions; that don’t take into account the whole human condition?
These citizens deserve a serious, targeted public health intervention. Neighborhoods that have been displaced, disrupted, and left with major health inequities cannot be expected to thrive without local investment and attention. What we learned from our interviews led to recommendations that should be used to augment SUD services that can better meet this population’s specific needs and, ultimately, allow treatment and recovery services to become more inclusive and serve a wider community. Mahatma Gandhi reminded us that “the true measure of any society can be found in how it treats its most vulnerable members,” and in that vein, the evaluation of public health can be appraised by how well we care for our most vulnerable populations. It's clear that the City of Rochester, Monroe County, and local substance use programs have more work to do on issues of inclusion in our community before presenting themselves for such an appraisal.
REFERENCES:
MEETING THE TREATMENT AND RECOVERY NEEDS OF WOMEN
Bailey, K., Trevillion, K., & Gilchrist, G. (2019). What works for whom and why: A narrative systematic review of interventions for reducing post-traumatic stress disorder and problematic substance use among women with experiences of interpersonal violence. Journal of Substance Abuse Treatment, 99, 88-103. https://doi.org/10.1016/j.jsat.2018.12.007
Center for Substance Abuse Treatment. (2009). Substance Abuse Treatment: Addressing the Specific Needs of Women. Treatment Improvement Protocol (TIP) Series 51. HHS Publication No. (SMA) 09-4426. Rockville, MD: Substance Abuse and Mental Health Services Administration. https://www.ncbi.nlm.nih.gov/books/NBK83252/pdf/Bookshelf_NBK83252.pdf
Dansky, B. S., Saladin, M. E., Brady, K. T., Kilpatrick, D. G., & Resnick, H. S. (1995). Prevalence of victimization and posttraumatic stress disorder among women with substance use disorders: Comparison of telephone and in-person assessment samples. International Journal of the Addictions, 30(9), 1079-1099.
Greenfield, S. F. (2016). Treating women with substance use disorders: The women's recovery group manual (1st ed.). The Guilford Press.
Greenfield, S.F.,, Back, S. E., Lawson, K., & Brady, K. T. (2010). Substance abuse in women. The Psychiatric Clinics of North America, 33(2), 339-355. https://doi.org/10.1016/j.psc.2010.01.004
Kim, T. W., Saitz, R., Cheng, D. M., Winter, M. R., Witas, J., & Samet, J. H. (2012). Effect of quality chronic disease management for alcohol and drug dependence on addiction outcomes. Journal of Substance Abuse Treatment, 43(4), 389-396. https://doi.org/10.1016/j.jsat.2012.06.001
Knight, K. R. (2015). Addicted.pregnant.poor. Duke University Press. https://doi.org/10.1215/9780822375180
Morse, D. S., M.D, Cerulli, Catherine, J.D., Ph.D, Bedell, P., M.A, Wilson, J. L., Thomas, K., Mittal, M., Ph.D, Lamberti, J. S., M.D, Williams, Geoffrey, M.D., Ph.D, Silverstein, J., B.S, Mukherjee, A., B.A, Walck, D., M.S, & Chin, N., Ph.D. (2013;2014;). Meeting health and psychological needs of women in drug treatment court. Journal of Substance Abuse Treatment, 46(2), 150-157. https://doi.org/10.1016/j.jsat.2013.08.017
Saladin, M. E., Brady, K. T., Dansky, B. S., & Kilpatrick, D. G. (1995). Understanding comorbidity between ptsd and substance use disorders: Two preliminary investigations. Addictive Behaviors, 20(5), 643-655. https://doi.org/10.1016/0306-4603(95)00024-7
Simpson, T. L., Rise, P., Browne, K. C., Lehavot, K., & Kaysen, D. (2019). Clinical presentations, social functioning, and treatment receipt among individuals with comorbid life‐ time PTSD and alcohol use disorders versus drug use disorders: Findings from NESARC‐III. Addiction (Abingdon, England), 114(6), 983-993. https://doi.org/10.1111/add.1456
MEETING THE TREATMENT AND RECOVERY NEEDS OF MEN
Boeri, M., Gardner, M., Gerken, E., Ross, M., & Wheeler, J. (2016). “I don’t know what fun is”: Examining the intersection of social capital, social networks, and social recovery. Drugs and Alcohol Today, 16(1), 95-105. https://doi.org/10.1108/DAT-08-2015-0046
Center for Substance Abuse Treatment. (2009). Substance Abuse Treatment: Addressing the Specific Needs of Women. Treatment Improvement Protocol (TIP) Series 51. HHS Publication No. (SMA) 09-4426. Rockville, MD: Substance Abuse and Mental Health Services Administration. https://www.ncbi.nlm.nih.gov/books/NBK83252/pdf/Bookshelf_NBK83252.pdf
Cloud, W., & Granfield, R. (2008). Conceptualizing recovery capital: Expansion of a theoretical construct. Substance use & Misuse, 43(12-13), 1971-1986. https://doi.org/10.1080/10826080802289762
Common Ground Health. (n.d.) Opioid Overdose Rates by Race/Ethnicity and Socioeconomic Status New York Finger Lakes Region. Retrieved from: https://www.commongroundhealth.org/insights/library/opioid-overdose-rates-by-raceethnicity-and-socioeconomic-status
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245-258. https://doi.org/10.1016/S0749- 3797(98)00017-8
Hamm, J.A. (2018). Addicts Speak: An Exploratory Ethnographic Study of Opioid Addiction. Bucknell University Honors Thesis. Bucknell Digital Commons. https://digitalcommons.bucknell.edu/honors_theses/465/
Hennessy, E. A. (2017). Recovery capital: A systematic review of the literature. Addiction Research & Theory, 25(5), 349-360. https://doi.org/10.1080/16066359.2017.1297990
Herbeck, D.M., Brecht, M.L., Christou, D. and Lovinger, K. (2014). A qualitative study of the methamphetamine users’ perspectives on barriers and facilitators of drug abstinence. Journal of Psychoactive Drugs, 46(3), 215-225.
Latino Health Coalition. (n.d). YPLL Disparity by Cause of Death, Latino vs White (not Latino) New York Finger Lakes Region (2013 - 2015). Common Ground Health. Retrieved from: https://www.commongroundhealth.org/insights/library/ypll-disparity-by-cause-of-death-latino-vs-white-not-latino
McKay, J. R. (2017). Making the hard work of recovery more attractive for those with substance use disorders. Addiction (Abingdon, England), 112(5), 751-757. https://doi.org/10.1111/add.13502
Monroe County Heroin Task Force. (n.d.). Retrieved from: https://www.monroecounty.gov/sheriff-heroin-task-force
Zschau, T., Collins, C., Lee, H., & Hatch, D. L. (2016). The hidden challenge: Limited recovery capital of drug court participants' support networks. Journal of Applied Social Science, 10(1), 22- 43. https://doi.org/10.1177/1936724415589633
In The News

WHAM: Study looks at factors behind opioid epidemic in Rochester

WXXI: How has the opioid epidemic affected communities of color?

Spectrum: Law enforcement, local advocacy center battling opioid crisis in Rochester